The current gold standard for detecting prostate cancer is a Systematic Transrectal Ultrasound (TRUS) Biopsy. For the last 30 years TRUS Biopsy has changed very little where 12 or more needle biopsy samples are extracted from the prostate.
The procedure is performed using an ultrasound through the rectal wall (transrectal) and the targeting is based on random sampling in different sections of the prostate. In essence, it is a blind biopsy procedure and there is a high rate of false negatives (cancer is present but biopsy is negative) and inadequate sampling of cancer using this procedure. It can also detect low volume, low grade insignificant cancer that will often lead to unnecessary treatment.
Systematic TRUS prostate biopsies can miss clinically significant cancer in up to one third of men. Often, repeat TRUS biopsy sessions will not yield a positive diagnosis and cause unnecessary delay and worry. That is because 30-40% of prostate cancer is located in the anterior, midline (transitional zone), or apex of the gland, areas that are not routinely sampled by TRUS biopsy.
The alternative is a transperioneal mapping biopsy that requires general anesthesia, is usually performed in a hospital, with as many as 80-100 or more separate biopsies to effectively sample the entire gland. You can think of this as playing the game “Battleship” where you cannot see your opponents ships and every square needs to be sampled to determine the location, size and type (grade) of ships (cancer). Unlike the game, with transperioneal biopsy you don’t get immediate results as you select each square.
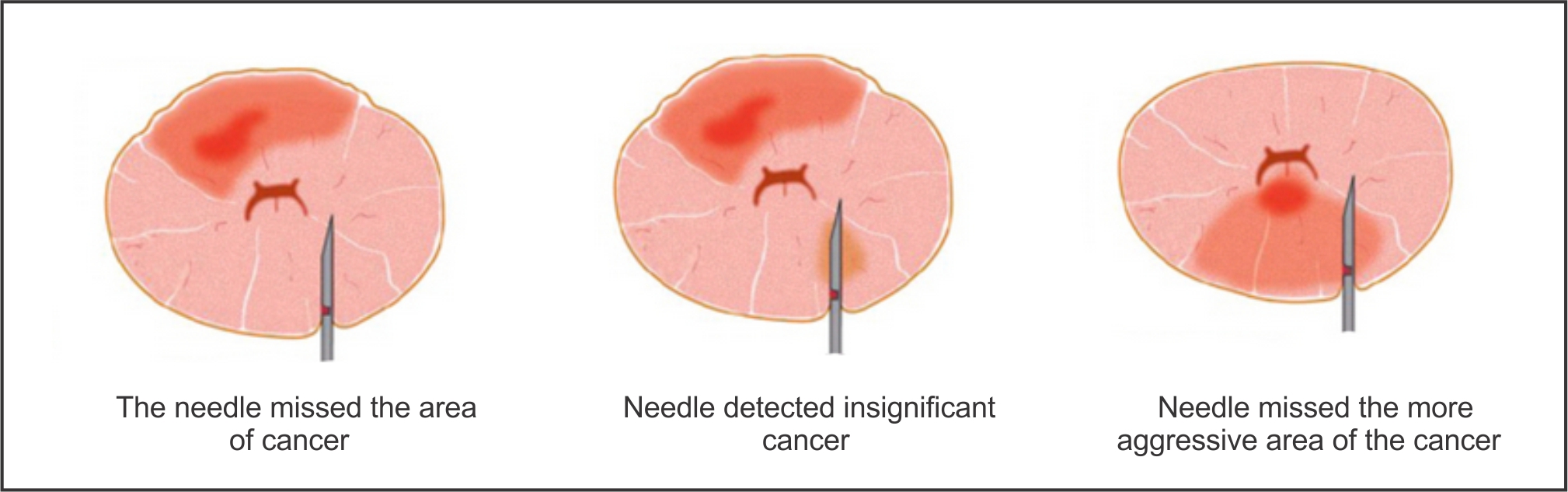
The figures below illustrate common problems of a traditional TRUS biopsy.
Many of these problems are solved with the use of Multiparametric 3T MRI of the kind that is provided by Partners Imaging Centers. An MRI will often determine whether a biopsy is necessary in the first place or whether there is significant disease.
If a significant cancer is suspected, MRI provides a method to target the suspicious area on biopsy with better results compared to performing a ‘blind’ biopsy. Many physicians are now ordering a multiparametric 3T MRI prior to a biopsy and will rely on the MRI images and prostate localizing map that we draw with each positive MRI exam, to use what’s called “cognitive fusion.” Prior to the TRUS biopsy they will review the MRI images and map to direct the biopsy to the location of the suspected tumor.
The picture to the left shows an MRI image of the prostate that has been contoured (green line) to identify the prostate gland and a region of interest circled (red line) identified as a possible cancer.
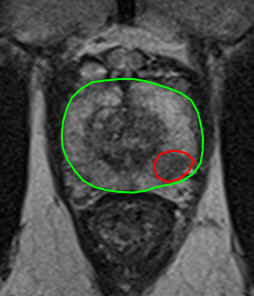
With the benefit of this MRI and contouring, your urologist now has a much greater probability of obtaining meaningful biopsy samples compared to random sampling.
As of 2016, there are a small number of companies that now offer a targeted biopsy solution. This operates by ‘fusing’ images from an MRI with ultrasound images. The fused images provide a 3D picture for the urologist and the targeting mechanism. In most cases, only a few biopsy cores are needed such is the accuracy of the procedure. An MRI of the prostate followed by a targeted 3D MRI/US Fusion Biopsy can significantly increase detection, grading, and staging of disease.
The fusion of MRI with Ultrasound images is a technology that is rapidly improving. The images that Partners Imaging provides can work with all of the companies developing this targeted solution.
Partners Imaging can guide you to physicians that are currently using MRI targeted biopsy technology. It is widely believed that targeted prostate biopsies will become the gold standard and replace the random TRUS biopsy.
.